
jueves, 13 de junio de 2013
Orotic Aciduria.
Autosomal recessive condition where there's a defect in the enzyme Orotate Phosphoribosyltransferase or Orotidine 5'-phosphate descarboxylase.
The abnormal functioning of either of these enzymes promotes the accumulation of Orotic Acid. This is important cause Orotate is the precursor of the Novo synthesis of Pyrimidines, process where it converts to UMP (Uridine Monophosphate)
{kind=link}
The findings are:
- High levels of Orotic Acid in the urine.
- Megaloblastic Anemia (non responsive to administration of B12 nor Folic Acid).
- Failure to thrive.
- NO hyperammonemia (feature that makes the distinction between OTC deficiency and this condition)
(*You guys should investigate a bit about OTC deficiency and find out what's going on there*).
The treatment is as simple as it gets, oral administration of URIDINE. So you're basically just going over that step.
Keep Studying!
sábado, 17 de marzo de 2012
Recordando un poco de Inmunología.
A propósito de que este semestre estamos cursando la materia de Reumatología y hemos tenido que desempolvar nuestros conocimientos sobre inmunología básica para comprender de mejor manera las alteraciones que ocurren en las enfermedades autoinmunes que afectan el sistema músculo-esquelético; pues se me ocurrió que sería bueno sacar nuevamente el tiempo para escribir un post aquí y hacerlo sobre los aspectos básicos inmunológicos que estamos supuestos a saber.
No voy a seguir necesariamente un orden lógico sino presentando datos básicos y específicos:
No voy a seguir necesariamente un orden lógico sino presentando datos básicos y específicos:
- La activación de los receptores de Linfocitos T (T Cell Receptor o TCR) y receptores de Linfocitos B (B Cell Receptor o BCR) conlleva a la activación del sistema intracitoplasmático y de cascada en el que se incluyen los ITAMs (Imunoreceptor Tyrosine-based Activation Motifs) : PTK, Zap-70. Estos motifs son inhibidos por los ITIMs (Inmunoreceptor Tyrosine-based Inhibition Motifs). Y la importancia de saber esto es que hay patologías de deficiencia inmunitaria en el que el fallo se encuentra en la ausencia o mal funcionamiento de algún ITAM o ITIM. Uno de las enzimas intracitoplasmáticas importantes en el caso de los Linfocitos T, es la calcineurina, ya que esta es la que inhibe el fármaco inmunosupresor Ciclosporina.
- Las citoquinas activan las células a través de receptores que utilizan Janus Kinases (JAKs) y STATs (Signal transducers and activators of transcription). Nuevamente, fallos en estos mecanismos pueden desequilibrar la respuesta inmune.
- Los linfocitos CD4 + solo pueden unirse al Complejo Mayor de Histocompatibilidad tipo II (MHC II) y los linfocitos CD8 + se unen al Complejo Mayor de Histocompatibilidad tipo I (MHC I). El MHC I presenta los antígenos por medio de la vía endógena mientras que el MHC II utiliza la vía exógena; en este proceso, la cadena invariante (CLIP) evita que ambas vías se mezclen con excepción de algunas células dendríticas. El HLA-DM se encarga de remover el CLIP y que se presente el antígeno.
- Los linfocitos B pueden ser activados de manera directa por el antígeno mientras que las células T solo pueden activarse cuando se les presenta el antígeno. Las células fagocitadoras son los Neutrófilos, Macrófacos y Células Dendríticas.
- El TCR se compone de cadenas alfa/beta o gamma/delta. La combinación alfa/beta predomina en la mayoría de ellos y una alteración mínima en ella puede tornarlos completamente afuncionales. El TCR debe ser coestimulado. Esto lo hace el CD28 de la superficie de las células T que se une al CD80 en la superficie de la célula presentadora de antígeno (APC); es decir, el TCR no se activa sin que se unan el CD28 con el CD80. El CTLA-4 en la superficie de la célula T se une también al CD80 e inhibe la coestimulación cuando es necesario regular a la baja la respuesta. El fármaco Abatacept bloquea la activación de CD28 y se emplea en artritis.
- Los Natural Killers son considerados como parte de la inmunidad innata porque no poseen o experimentan el proceso de recombinación de genes que ocurre en los linfocitos T y B, que les permite reconocer un montón de antígenos.
- En el proceso de maduración, los linfocitos T primero son Doble Negativos, lo que significa que no tienen ni CD4 ni CD8. Luego se convierten en Doble Positivos y poseen ambos CD4 y CD8, en este punto son puestos a prueba para ver si reconocen una molécula de MHC en un proceso que se denomina Selección Positiva y a través del cual, dependiendo de lo que reconozcan, se convierten en Positivos Únicos ya sea CD4 + o CD8+. Las células que reconozcan auto antígenos son eliminadas en el proceso de Selección Negativa por medio de la Tolerancia Central; este es un mecanismo fundamental en la prevención de autoinmunidad. La Tolerancia Periférica es llevada a cabo por los Linfocitos T reguladores (Treg) por medio del gen Fox p3 y también por muerte celular programada a través del Fas/ Fas Ligando (Fas/ FasL).
- Los linfocitos Th1 promueven la inmunidad celular al producir IFN-y con lo que amplían la función de los macrófagos y la expresión de MHC-I. Los linfocitos Th2 promueven la inmunidad humoral, luchan contra las alergias e infestación helmítica. Los Th2 producen IL-4, IL-10 e IL-5, que se oponen a los efectos del IFN-y, aumentan la producción de Ig-E. Debemos recordar también el otro subtipo de Linfocitos Th, llamados Th17.
- Los linfocitos CD8+ actúan por medio la de la Porfirina y las Granzimas. La Porfirina crea un poro en la membrana celular de la célula a atacar y permite que vesículas llenas de Granzimas entren a la célula y como las Granzimas son realmente proteasas, éstas terminan activando Apoptosis.
- Las Inmunoglobulinas consisten de dos cadenas Ligeras y dos cadenas Pesadas. Las Ligeras son kappa y lambda mientras que las Pesadas pueden ser Mu, Alfa, Delta, Epsilon y Gamma (IgM, IgA, IgD, IgE e IgG). Hay 4 tipos de IgG y 2 tipos de IgA. IgM forma un multímero e IgA forma un dímero. Las cadenas Ligeras son la región variable y las Pesadas son constantes y por eso son las que les dan el nombre a la Inmunoglobulina; la cadena constante posee la región Fc que se une al receptor Fc en las células fagocíticas o el complemento.
- Los linfocitos B experimentan reorganización de genes de su región VDJ o Variable Diversity Junction; estas representan 3 regiones diferentes en los genes. Para formar la cadena Pesada, la D y la J se unen y luego se les une la V; así que las células pro-B son células que aún no tienen cadena pesada mientras que las pre-B sí las tienen. Una vez que la cadena Pesada está lista, se inician señalizaciones para promover el rearreglo de la cadena Ligera y formar linfocitos B Inmaduros que solo poseen IgM, estos se conviertene en Maduros cuando tienen IgM e IgD en su superficie. Las linfocitos B también pueden convertirse en Linfocitos B de memoria o en células Plasmáticas, que son Linfocitos B que no poseen CD20; lugar de acción del Rituximab.
- El receptor de células B consiste en una IgM con cadenas alfa y beta. Hay que recordar que el BCR no solo recibe señales de proliferación sino que también internaliza antigeno para presentarlo y activar Linfocitos CD4. El BCR utiliza en su cascada de quinasas, a la Bruton tirosin kinase o BTK y la deficiencia de esta produce Agammaglobulinemia ligada a X.
- La hipermutación somática se refiere a la formación de Linfocitos B con una mayor afinidad para los antígenos, y se logra mediante mutaciones ampliadas y por ende, mayores cambios en los genes de las cadenas ligeras.
Espero que les sirva, la idea es que puedan volver a leerlo cada vez que necesiten recordar algo de esto.
domingo, 2 de octubre de 2011
Cervical Cancer in Developing countries / Cáncer de Cervix en países en desarrollo.
Cervical Cancer in Developing countries.
As most definitions refer, Cervical Cancer can be detected by a PAP smear. Nevertheless, most countries with poor and middle incomes do not have the resources or technology to perform such tests.
This is an important issue, because it is precisely in this countries where women with the major risks factors reside. We are talking about HPV infection, smoking, young age at the first full-term pregnancy, multiple full-term pregnancies, diet, poverty, oral contraceptives, Chlamydia infections, and others.
 For the year 2000, the incidence rate in Dominican Republic was about 38,4% with a death rate of 15,8%, according to a complete inform released by the PAHO on Cervical Cancer in Latin America and the Caribbean.
For the year 2000, the incidence rate in Dominican Republic was about 38,4% with a death rate of 15,8%, according to a complete inform released by the PAHO on Cervical Cancer in Latin America and the Caribbean. This article published in the New York Times caught my eye, and it was indeed incredibly interesting. It is called "Fighting Cervical Cancer with Vinegar and Ingenuity". It's about the implementation of an alternative way to detect Cervical Cancer in Asian countries, specifically Thailand. This practice is being taught to nurses in order to cover a great amount of women and make sure this process is accessible to most of them.
This alternative way is cheap, affordable, and most importantly ¡IT WORKS!. Yes, is Vinegar, as simple as it sounds. Here's some background "...developed by experts at the Johns Hopkins medical school in the 1990s and endorsed last year by the World Health Organization, brush vinegar on a woman’s cervix.".
Other advantage is that the patient can know right away whether everything's ok or she'll need treatment. Even greater, she can be treated right away as well, using cryotherapy (in this case with Carbon Dioxide CO2). This can definitely change the course of gynecological medicine in developing countries.
*Read the article by clicking on it's tittle*
Cáncer de Cervix en países en desarrollo.
Como refieren la mayoría de las definiciones, el cáncer cervical puede ser detectado por una prueba de Papanicolaou. Sin embargo, la mayoría de los países de bajos y medios ingresos, no tienen los recursos ni la tecnología para realizar tales pruebas.
Este es un tema importante, porque es precisamente en estos países donde la mayoría de mujeres con factores de riesgos residen. Estamos hablando de la infección por VPH, el tabaquismo, la edad joven en el primer embarazo a término, múltiples embarazos a término, la dieta, la pobreza, los anticonceptivos orales, las infecciones por Chlamydia, y otros.
Para el año 2000, la tasa de incidencia en la República Dominicana se estimaba en 38,4%, con una tasa de mortalidad del 15,8%, según un completo informe publicado por la OPS sobre cáncer cervicouterino en América Latina y el Caribe.
Un artículo publicado en el New York Times me llamó la atención, y si resultó ser muy interesante. Se titula "Lucha contra el cáncer de cuello del útero con vinagre e ingenio". Se trata de la implementación de un método alternativo para detectar el cáncer cervical en los países asiáticos, en particular Tailandia. Esta práctica se enseña a las enfermeras a fin de cubrir una gran cantidad de mujeres y asegurarse de que este proceso sea accesible para la mayoría de estas.
Este método alternativo es barato, asequible, y lo más importante ¡FUNCIONA!. Sí, vinagre, tan simple como suena. Aquí hay algunos antecedentes "...desarrollado por expertos en la escuela de Medicina John Hopkins en la década de 1990 y aprobado el año pasado por la Organización Mundial de la Salud, cepillar vinagre en el cuello uterino de una mujer.".
Otra ventaja es que la paciente puede saber de inmediato si todo está bien, o si necesitará tratamiento. Aún mejor, puede ser tratada de inmediato con crioterapia (en este caso con dióxido de carbono CO2). Esto definitivamente puede cambiar el curso de la medicina ginecológica en los países en desarrollo.
*Lea el artículo haciendo clic en el titulo*
“El Cáncer cervicouterino se puede
prevenir y curar a un costo y riesgo bajos
cuando el tamizaje para facilitar la
detección oportuna de lesiones precursoras,
está disponible junto con el diagnóstico
apropiado, el tratamiento y seguimento.”
Extraído de Cáncer Cervicouterino en América Latina y el Caribe. OPS
domingo, 11 de septiembre de 2011
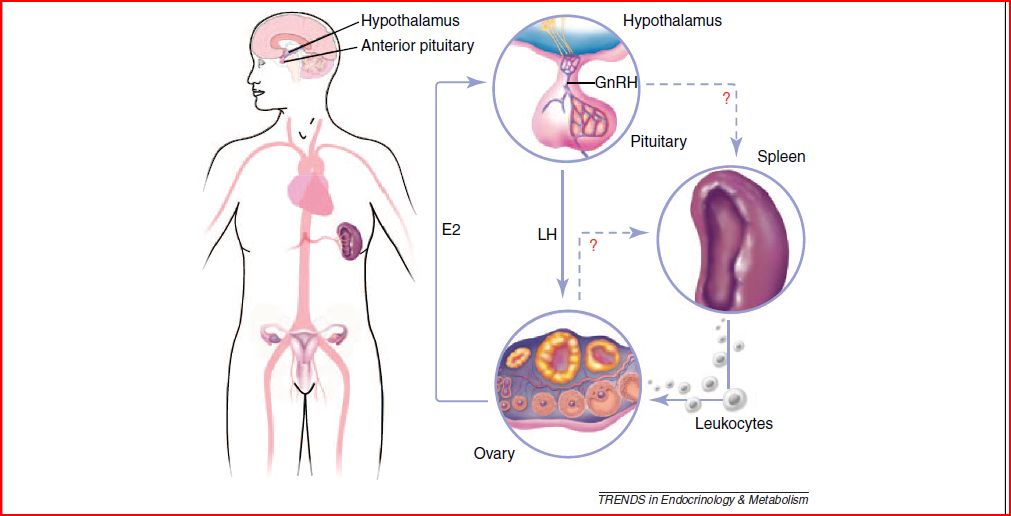
The Spleen and Ovulation
At the start of my college education while taking Biology, I was briefly introduced into a very light "view" of what goes on in a woman's body during the ovulation and menstruation period and it may seem corny, but the ability to give life that women posses is just incredible right from the start and lately, I have been reminded of this awesome capacity by some recent births (wich hands down, I'm sure will be some kick ass babies in no time!). A couple of years ago during our Physiology courses, we entered the world of Endocrinology wich included the Female Sex Hormones and that became a pretty exciting topic for me since this time around I had the chance to get a more in depth view on this subject, however the same way that it happens with a bunch of stuff in the Medicine world, a lot of things still go unanswered when it comes to the ovulation phase.
So a couple of days ago, I was "wasting time" jumping through some medical news headlines and I ended up in an Endocrinology journal since we are taking that subjec this semester ( from the specialty point of view now), And I ended up finding a review article relating the Ovulation period with the Spleen and Leukocytes, (yes, feel free to read that again). I know that this may not be news to some of you, since this research has been going on for the last decade but I really wanted to share this approach.
It turns out that there seems to be another key element in order for ovulation to take place other than the hormonal changes and that's where Inflammation comes in. There's actually a lot of info out there about pathological inflammation but it's the opposite when it comes to physiological scenarios of inflammation, wich means the details of how it works on the ovary are a little blurry. There is a breaktrough approach that has allowed advances in this field, and that's flow cytometry, wich now allows us to see exactly wich cell types are located on an specific site of the body, that's how researches ended up finding leukocytes inside the ovary prior and during the ovulation period.
Taking this into consideration, when I say inflammation I'm taking about the whole package: neutrophils, mast cells, eosinophils, macrophages, NK cells and lymphocites. But they've already gone farther by discovering specific functions for these guys with neutrophils and lymphocites having a role in luteal formation, neutrophils also play part in follicle maturation and ovulation and mast cells, eosinophils and neutrophils dealing with ECM degradation. Meanwhile, NK cells are relevant for angiogensis and macrophages secret IL-8 enhancing chemotaxis.
But how does this happen and where do these guys come from? The current hypothesis is that it happens via the same Hypothalamous-Pituitary-Ovarian axis that we should be familiar with but there's a twist to it and that's where the Spleen comes in. And isn't the spleen supposed to be some non functional purple organ that functions as a cell cementery in our bodies? Well, for females the answer now seems to be NO.
Recent studies, using the above mentioned flow cytometry have demostrated that after a heart attack, the spleen starts sending out armies of leukocytes to deal with the inflammation inside the heart. The same approach was used to asses the procedence of leukocytes arriving at the ovary during the pre-ovulatory and ovulation period and they ended up seeing that as the ovarian vessels start filling up with these inflammatory cells, the spleen's population of leukocytes starts decreasing. Up to this point, it is thought that the LH hormone is the one responsible for going up to the hypothalamous and triggering the send me some white cells!!! signal moments prior to the start of ovulation and even if the above has been tested, it is in the triggering mechanism of this physiological inflammation where most questions remain.
There is a simple question that should arise from this: then does this mean that women who go trough splenectomy should be considered infertile? The problem is that along with splenectomy comes a process of radiotherapy and chimiotherapy wich could alone be harmful to the female reproductive abilities and it's difficult to measure this effect on humans. However, studies in animals who have gone trough splenectomy show that the ovulatory becomes irregular and some of them actually stop ovulating all together. Another intriguin fact is that, considerably large leukocytes populations have been spotted in other female reproductive organs such as the uterus and flow cytometry shows that not all of the leukocytes coming out from the spleen end up in the ovary wich could also mean that at the same time they end up somewhere else in the reproductive tract.
Seems like we'll have to start thinking of ovulation as an important inflammatory event in no time and that's where the bridge between immunology and reproductive sciences will have to keep being crossed. This promises to be an interesting ride!
lunes, 29 de agosto de 2011
CPAP in newborns.

Before further ado, I'll go ahead and let you guys know that CPAP means Continuous Positive Airway Pressure.
First time I heard about it was regarding Sleep Apnea, that article expressed that CPAP was a valuable treatment for it, along with weight loss and other adjustments of course. Well, after a while of that and without hearing the word CPAP again, it was brought up today in our Pediatrics and Childcare class.
It caught my attention cause our teacher mentioned that the childcare unit of our regional public hospital was going to received some of these devices. She was so excited while mentioning it and I just couldn't get it, I thought she was all "we're going to receive something new! Wee!" but after reading about the use and advantages of the CPAP in newborns that are either pre-term or just with breathing issues, I finally got her, most of all the potential advantages it has in developing countries like ours. This article explains how the use of CPAP for primary management of RDS (Respiratory Distress Syndrome) allows patients to save money by not starting treatment with SRT (Surfactant Replacement Therapy) and instead using it in non-responders to CPAP
 Might sound unimportant to some people or just something already known and re-known for that matter, well yes, I'm not going to argue with that, it's not a new therapy so private clinics already have them. Usually money it's not an issue for those who attend to private clinics, they can pay for their services or they have a pretty good insurance but the reality of the poor part of society is completely different. Let me be breve and let you know about what public hospital means in "my language", it's a place/building the government has enabled with beds, some basic equipment (X-ray machine, EKG machine and others), doctors, nurses, residents, interns and med students.. everything else comes from your pocket, with that I mean "even the gauze" comes on your account. So, imagine that it must not be easy to have a newborn in NICU and be told what you need to do to keep your child alive but in the end you know you just don't have the means...
Might sound unimportant to some people or just something already known and re-known for that matter, well yes, I'm not going to argue with that, it's not a new therapy so private clinics already have them. Usually money it's not an issue for those who attend to private clinics, they can pay for their services or they have a pretty good insurance but the reality of the poor part of society is completely different. Let me be breve and let you know about what public hospital means in "my language", it's a place/building the government has enabled with beds, some basic equipment (X-ray machine, EKG machine and others), doctors, nurses, residents, interns and med students.. everything else comes from your pocket, with that I mean "even the gauze" comes on your account. So, imagine that it must not be easy to have a newborn in NICU and be told what you need to do to keep your child alive but in the end you know you just don't have the means... 360· and back to the essence of the subject, here are two pictures, one is a nasal-CPAP and the other is a helmet-CPAP, even if both of them do "the same" work, some authors have their preferences and the why's of it. But I'm not planning to get into that, here's and article that refers about it, there's more from where it came from =P, so I invite you to inform yourself a little about it.
Good Night!
Test de APGAR / APGAR Score
Es un test utilizado en neonatología, que persigue la valoración clínica del neonato. Ideado e implementado en 1952 por Virginia Apgar, el test consta de la valoración de 5 parámetros en una escala de medición 0-2 cada uno, siendo la puntuación final de 0 a 10. Debe realizarse el test al minuto de nacer y luego a los 5 minutos, la primera vez permite valorar la torancia del proceso de nacimiento, mientras que la segunda permite la valoración de la adaptabilidad y capacidad de recuperación.
The Apgar scoring is used to evaluate the newborn in a general matter. Virginia Apgar introduced this test in 1952. In order to perform it one must evaluate 5 simple criteria on a scale from 0-2, then summing up the five values, the resulting Apgar score ranges from 0 to 10. One must perform this test before1 minute after birth and then again 5 minutes later, the first time we assess the tolerance of the process of birth and the second time we assess the ability to adapt and capacity of recovery.
A - Appearance / Apariencia (Color of the skin / Color de la piel)
P - Pulse / Pulso (Cardiac Frequency / Frecuencia Cardiaca)
G - Grimace / Gesticulación (Reflexes / Reflejos)
A - Activity / Actividad (Muscular Tone / Tono Muscular)
R - Respiration / Respiración (Quality not frequency)


Conociendo el significado de las puntuaciones obtenidas:
Una puntuación de 8-10 = Buenas condiciones.
Una puntuación de 4-6 = Se necesita vigilancia y valoración clínica.
Una puntuación <4 = Considerada grave, se requiere ventilación y medicamentos IV.
Una puntuación de 0 = Probable muerte fetal/neonatal. Junsto a un Ph igual o < 7.
Getting to know the meaning of the scoring obtained:
A scoring of 7-10 = Considered normal, good conditions.
A scoring of 4-6 = Clinical watch and assessment needed.
A scoring below 4 = Considered an emergency, ventilation and IV medications required.
A scoring of 0 = Probable fetal/neonatal death. Along with a Ph lower or equal to 7.
Espero que disfrutaran la explicación y que la hayan comprendido, sino cualquier pregunta es bienvenida. Me parece que es buena idea tomarme el tiempo de escribir en ambos idiomas y así la información puede llegar a más personas =), ya el francés vendrá por ahí!.
I hope you guys enjoyed the explanation and most importantly understood it, if otherwise any question is welcome. I got to the conclusion that's a good idea to take some time and write both spanish and english, that way more people can get benefit from the information. Soon enough will come french =P.
Hasta la próxima / Until next time.
martes, 9 de agosto de 2011
Mini Mental Test de Folstein. Folstein Mini Mental State Exam(MMSE).
Es un test realizado principalmente en el área de neurología, con la finalidad de evaluar ciertos aspectos cognitivos del paciente, se basa en una puntuación de 30pts y puede realizarse en unos pocos minutos dependiendo de la experiencia con que cuente el evaluador.
El test consta de 11 pasos, una puntuación menor de 24 sugiere demencia; la misma tiene diferentes grados, entre 23-21 la demencia es leve, entre 20-11 nos encontramos frente a una demencia moderada y menor de 10 de una demencia severa. Aquí los puntos que debemos evaluar y cómo hacerlo.
Preguntar al paciente:
- El día de la semana (1).
- Fecha (número en el calendario) (1).
- Mes (1).
- Año (1).
- Estación del año (1).
2. Orientación en lugar (5pts)
Preguntar al paciente:
- Lugar de la entrevista (Planta o área del hospital) (1).
- Hospital (1).
- Ciudad (1).
- Provincia (1).
- País (1).
3. Registro de 3 palabras (3pts)
Se pide repetir 3 palabras, se otorga un punto por cada palabra que el paciente recuerde.
4. Atención y Cálculo (5pts)
Serie de 7. Pedir al paciente que reste 7 iniciando desde 100. Realizar 5 repeticiones, por cada correcta se otorga un punto. Ej. 100 - 7 = 93 - 7 = 86 - 7 = 79... Puede también pedirse al paciente que deletree la palabra MUNDO al revés. Ej. O - D - N - U - M.
5. Recall (3pts)
Se otorga un punto por cada palabra que el paciente recuerde de las 3 que se pidió memorizar en el paso 3.
6. Nominación (2pts)
Pedir al paciente que nombre dos objetos que serán mostrados, otorgar 1 punto por cada una que se responda correctamente.
7. Repetición (1pt)
Pedir al paciente que repita una de estas oraciones:
- Tres perros en un trigal.
8. Comprensión (3pts)
Indica al paciente que realice 3 acciones, por ejemplo: Tome este lápiz (1), colóquelo sobre la mesa (1), tómelo con la mano izquierda (1). O el clásico Tome este papel (1), dóblelo a la mitad (1), póngalo en el suelo (1).
9. Lectura (1pt)
Escribir una frase en un papel, pedir al paciente que la lea para él mismo y luego la realice. Ej. "Levante su mano derecha" o el clásico "Cierre los ojos"
10. Escritura (1pt)
Pedir al paciente que escriba una oración con sentido lógico.
11. Dibujo o destrezas visuoespaciales (1pt)
Realizar este dibujo y pedirle al paciente que lo copie al lado. Son dos pentágonos cruzados en las puntas.

Aquí les dejó unas páginas con unos buenos ejemplos y guías.
1. http://www.geroeducation.org/HyperText_Module/Delirium/html/mmse.htm
2. http://lifemanagement.com/nextsteps/Mini_Mental_Status_Exam.pdf
3. http://bit.ly/q4atrr
Suscribirse a:
Entradas (Atom)